The PAH heart and lung connection
Your heart and lungs work together to make sure that your body gets the oxygen it needs. Knowing how the heart and lungs work together as partners will help you understand what happens in your body when you have pulmonary arterial hypertension (PAH).
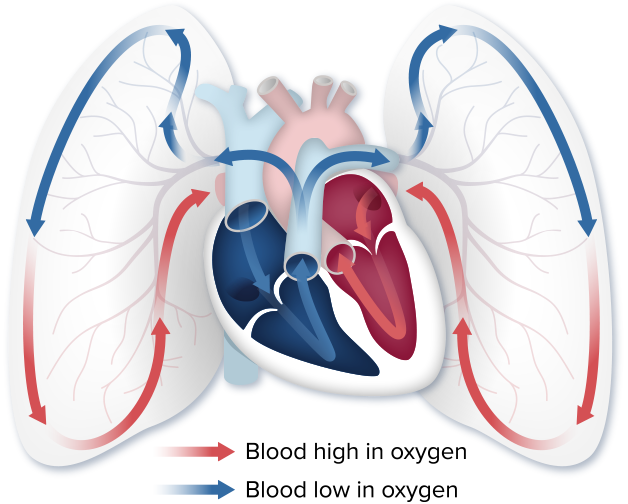
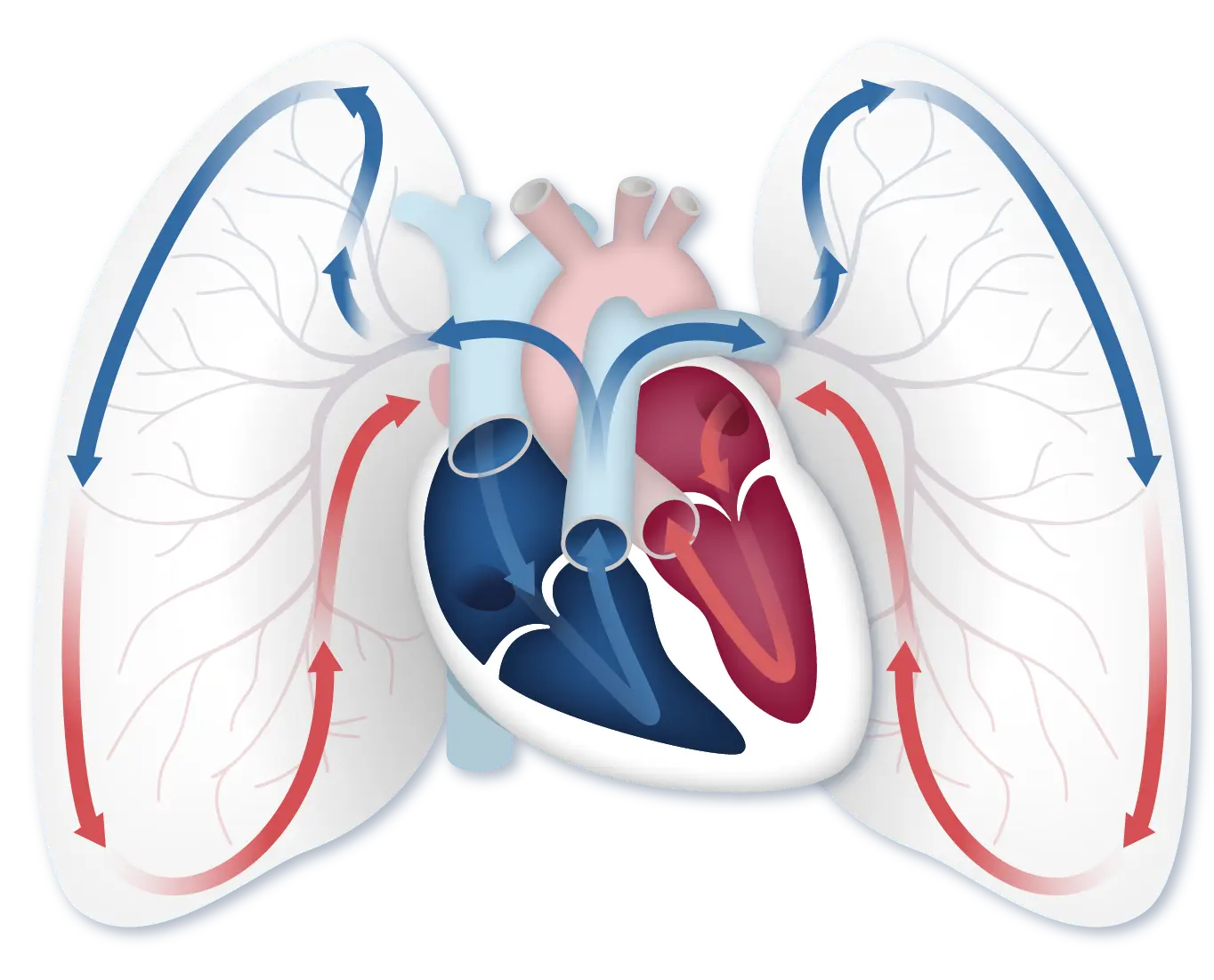
When you inhale, you breathe oxygen into your lungs. Blood flows from the heart to the lungs, where it picks up oxygen. The oxygenated blood goes back into the heart, where it is pushed out to the rest of the body.
When you have PAH, the blood vessels in your lungs thicken and become narrow, making the right side of your heart work harder to pump blood through them. This can cause serious, life-threatening changes to the right side of the heart and can even cause heart failure.

“The more I know about the right heart, the more I can visualize what’s happening inside my body.” —Thekla, PAH Initiative Patient Ambassador
A closer look at the heart
Each side of the heart has a specific job when it comes to getting your body the oxygen that it needs. Each side is built differently to best perform its job.
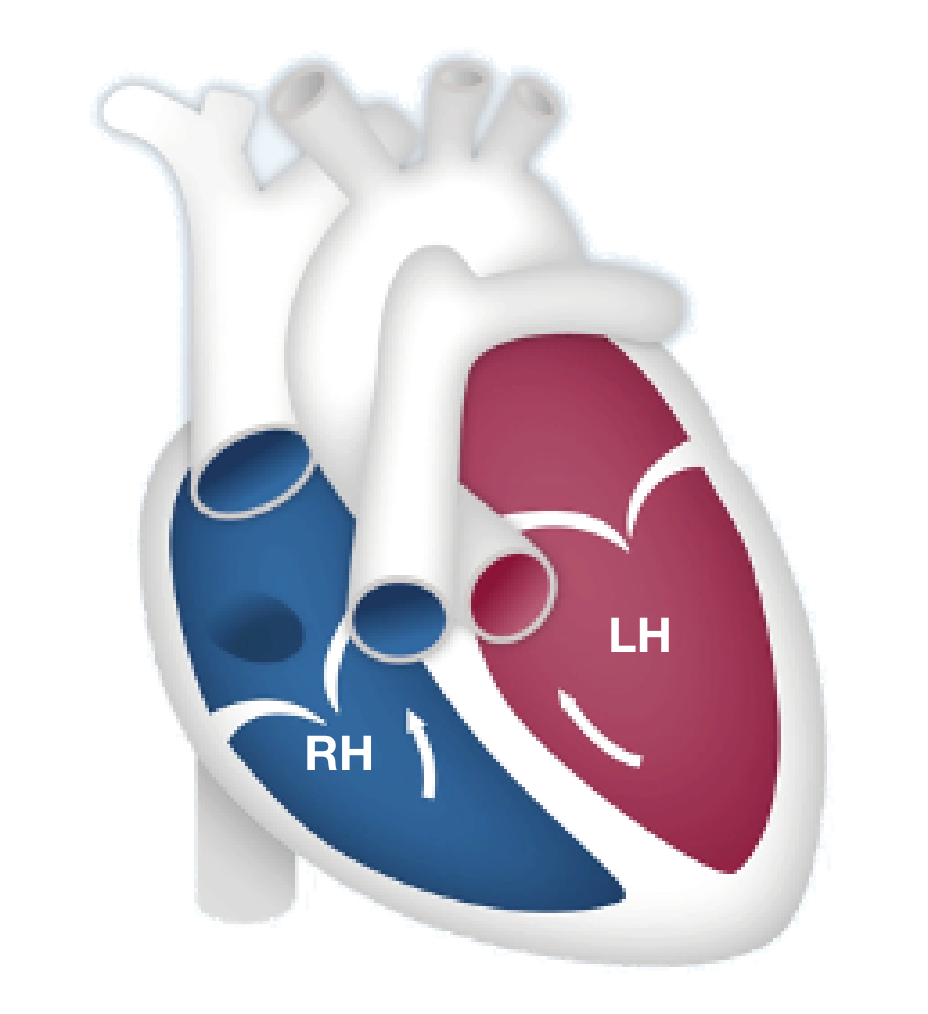
The right side of the heart is smaller and thinner because it is only meant to push the blood a short distance—from the heart to the lungs—to receive oxygen. The right side of the heart pumps blood into the blood vessels in your lungs. As blood flows through the lungs in these small vessels, red blood cells pick up oxygen from the air we breathe.
After the blood has received oxygen, it travels to the left side of the heart, which pumps that blood out to the rest of the body. The left side of the heart is larger and stronger than the right side because it has to push this oxygenated blood a long distance throughout the entire body.
PAH affects the right side of the heart
Now that we know a little more about how the heart and lungs work together, let’s talk about PAH.
PAH, a lung disease, is a specific type of high blood pressure that affects your heart and lungs. PAH begins when the walls of the lung’s blood vessels thicken and narrow. When this happens, it becomes harder for blood to pass through the vessels, and that means there is less blood flowing to the lungs. The reduced blood flow in the lungs creates pressure on the right side of the heart.
PAH can be confusing
This video explains the basics of PAH and how it affects the body. You’ll learn how PAH changes the heart and lungs, what happens as PAH progresses, and symptoms of PAH progression.
[Video title: PAH Basics, Part 1 in the PAH Initiative Video Series] Hi, I’m Dr Lana Melendres-Groves, a pulmonary arterial hypertension specialist and director of the pulmonary hypertension program at the University of New Mexico. I have been treating pulmonary diseases for over 12 years with a specialization in PAH for over 9 years. My clinic has treated over 5,000 patients and I currently oversee 250 PAH patients on PAH-specific medicines. In this video, we’ll cover the basics of pulmonary arterial hypertension, also known as PAH. Understanding what PAH is can be confusing because even healthcare providers may tell you different things about it. Some may say your heart doesn’t work as well as it needs to. It’s really about the blood vessels. The real problem is in the lungs or it’s just hypertension. This is why it’s so important to find an experienced PAH specialist to help you. A PAH specialist is a cardiologist or pulmonologist who has had specific training in PAH and understands how challenging this disease really is.
The heart, lungs, and blood vessels all work together as a cardiovascular team and PAH affects each of these vital organs. So let’s start with the heart. You may already know that the heart has 4 chambers. Two chambers are called atria and receive blood from the other parts of the body and the other 2 chambers are called ventricles and pump blood out of the heart. The right atrium receives blue, oxygen-poor blood from the body and the right ventricle pumps that oxygen-poor blood to the lungs where it can pick up oxygen. The left atrium receives red, oxygen-rich blood from the lungs and then the left ventricle pumps the oxygen-rich blood to the rest of the body. Although cardiac diseases, including heart attacks, are more common in the left ventricle, it’s actually the right ventricle that is affected in people who have PAH.
[End of video: PAH Initiative, Sponsored by United Therapeutics, Committed to Improving the Lives of Patients. For more resources about PAH, please visit www.PAHInitiative.com. Copyright 2019 United Therapeutics Corporation. All rights reserved.]
Think of PAH like construction on a highway
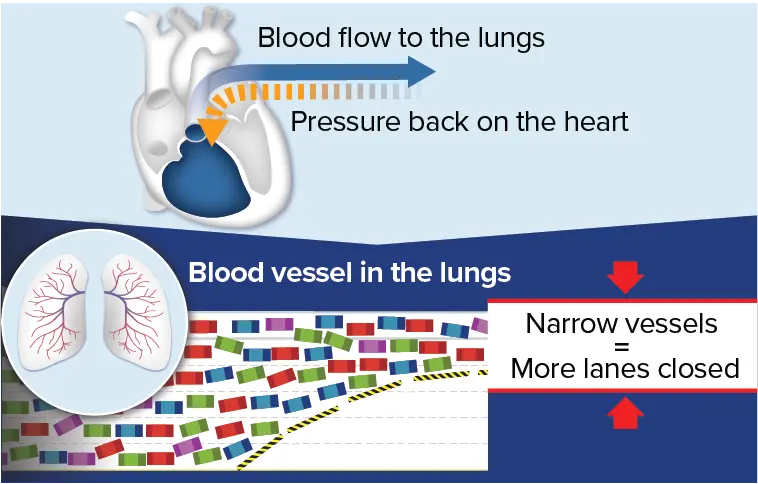
Imagine your blood vessels as the highway. Your blood cells are like the cars. When blood vessels in the lungs become narrow, the flow of blood cells is reduced—similar to the way traffic flow slows down when lanes are closed.
With PAH, the heart works harder
When blood vessels in the lungs narrow, the heart has to work harder to pump blood through the lungs to receive enough oxygen to be carried throughout the body.
The right side of the heart grows larger and more muscular as it pumps harder. This may sound like a good thing, but remember, the right side of the heart is not meant to work hard. It’s only meant to pump blood from the heart to the lungs. When it has to pump harder for a long period of time, the right side of the heart becomes damaged.
When the right side of the heart struggles to keep up, the rest of your body doesn’t get the oxygen it needs to function. This is when PAH symptoms often get worse.
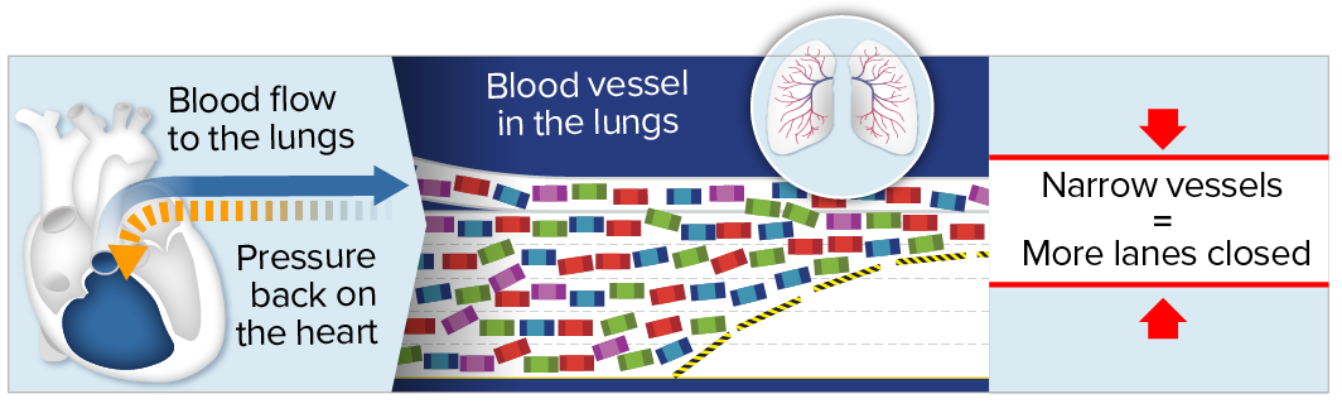 With PAH, narrowed blood vessels in the lungs cause blood flow to
slow down and back up, similar to traffic during construction on a
highway. This backup creates pressure, which strains the heart
over time.
With PAH, narrowed blood vessels in the lungs cause blood flow to
slow down and back up, similar to traffic during construction on a
highway. This backup creates pressure, which strains the heart
over time.
 With PAH, narrowed blood vessels in the lungs cause blood flow to
slow down and back up, similarly to traffic during construction on
a highway. This backup creates pressure, which strains the heart
over time.
With PAH, narrowed blood vessels in the lungs cause blood flow to
slow down and back up, similarly to traffic during construction on
a highway. This backup creates pressure, which strains the heart
over time.
Opening the blood vessels in the lungs reduces pressure on the heart
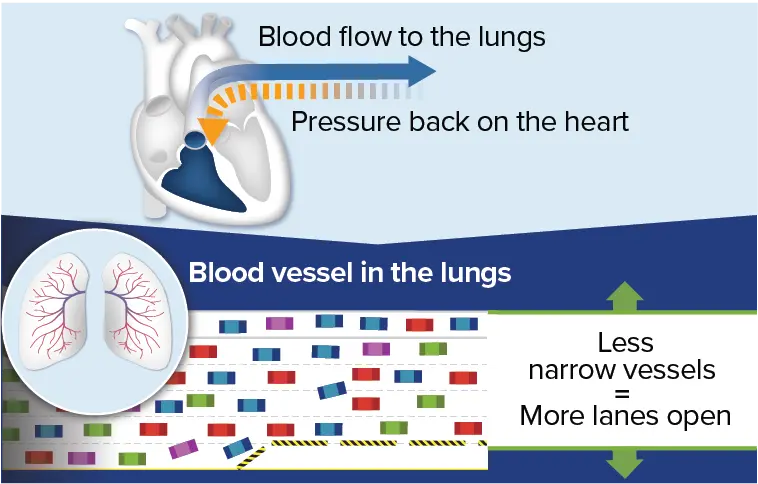
PAH medications help open up the “lanes” by giving the blood more space to flow through (for example, by making the blood vessels wider). Wider lanes help traffic (blood cells) move faster and more smoothly, with less backup. This means that the heart doesn’t have to work as hard to pump the same amount of blood through the lungs, and more oxygen can get to the rest of the body.
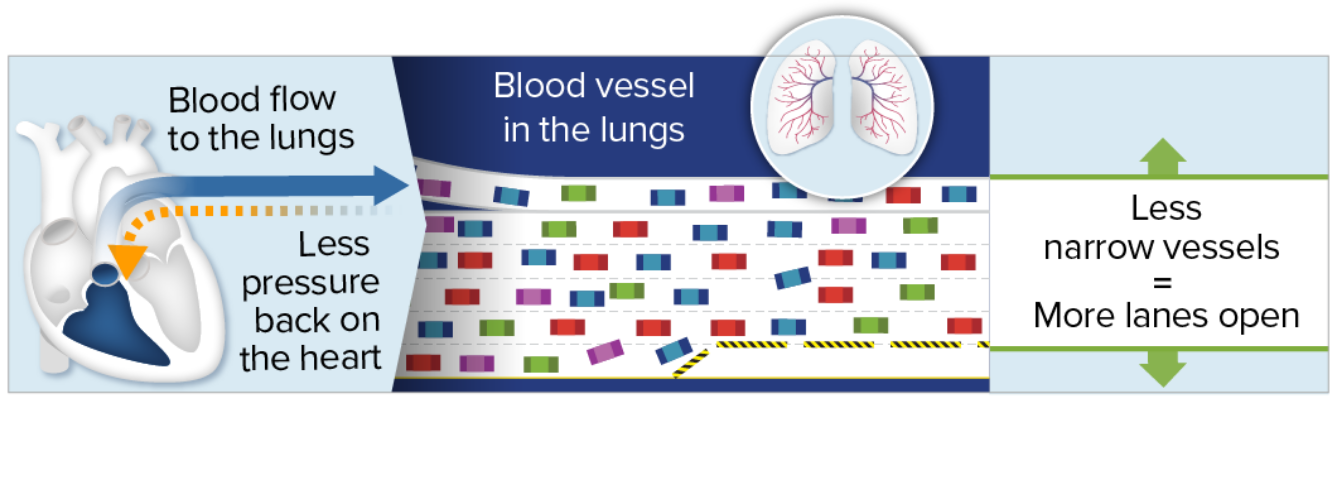 An important goal of treating PAH is to help the vessels in the
lungs widen to improve blood flow, similar to how traffic moves
faster when more lanes are open. Because the blood flows more
smoothly, there is less pressure and strain on the heart. Over
time, with less strain on the heart, symptoms may also
improve.
An important goal of treating PAH is to help the vessels in the
lungs widen to improve blood flow, similar to how traffic moves
faster when more lanes are open. Because the blood flows more
smoothly, there is less pressure and strain on the heart. Over
time, with less strain on the heart, symptoms may also
improve.
 An important goal of treating PAH is to help the vessels in the
lungs widen to improve blood flow, similarly to how traffic moves
faster when more lanes are open. Because the blood flows more
smoothly, there is less pressure and strain on the heart. Over
time, with less strain on the heart, symptoms may also
improve.
An important goal of treating PAH is to help the vessels in the
lungs widen to improve blood flow, similarly to how traffic moves
faster when more lanes are open. Because the blood flows more
smoothly, there is less pressure and strain on the heart. Over
time, with less strain on the heart, symptoms may also
improve.
What can monitoring the heart tell healthcare providers?
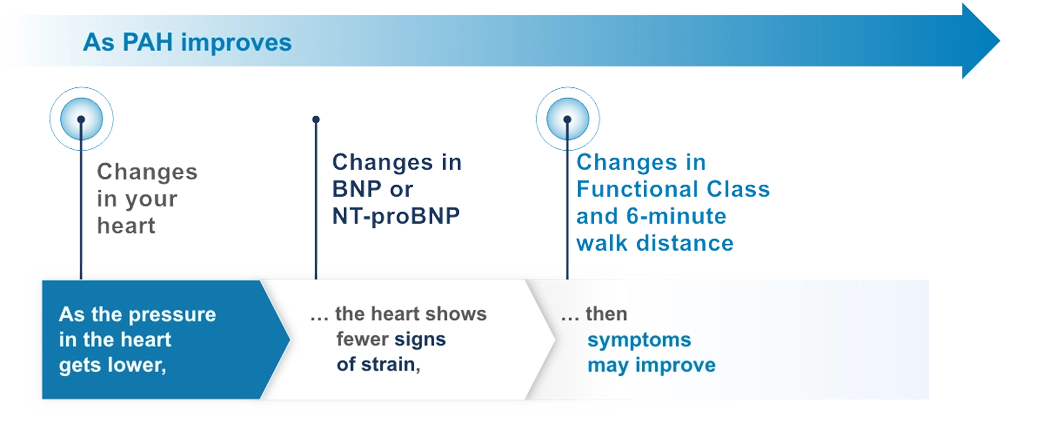
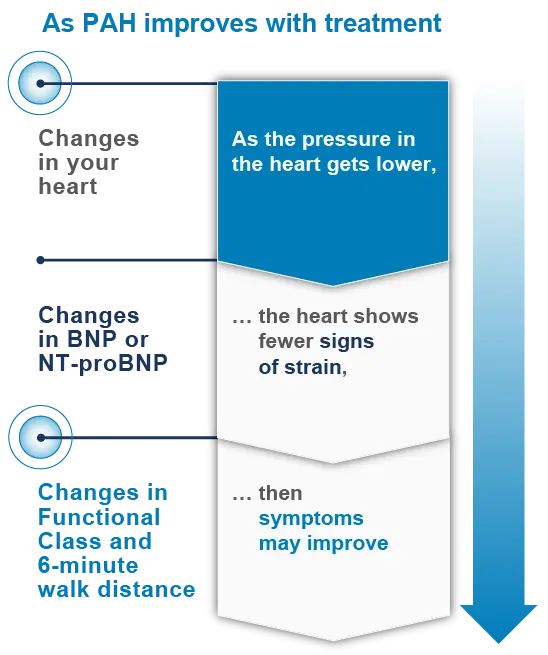
Changes in the heart can be an early sign that PAH is getting better or worse. This is because changes to your heart occur before your symptoms, including your Functional Class or 6-minute walk distance.
Because of this, changes in the heart can be an early signal to healthcare providers that treatment plan adjustments—such as PAH medications and lifestyle (diet and exercise) modifications—may be beneficial. Changes in the heart can also be an early signal that your treatment plan is working.
Changes in your heart occur before your symptoms change
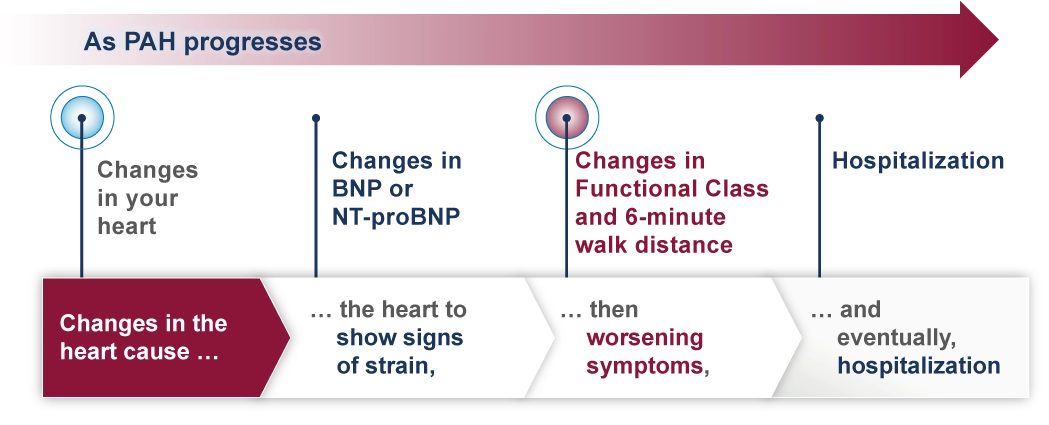
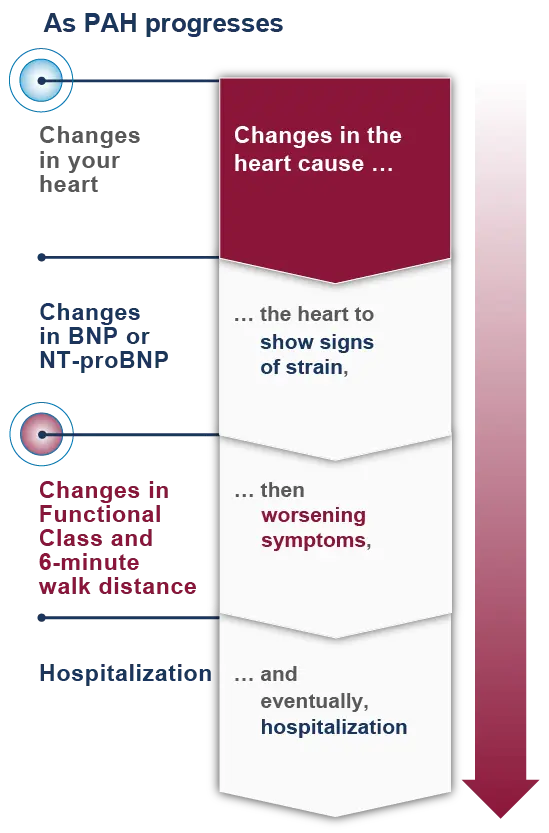
Changes to the heart occur before changes to biomarkers that can be monitored with blood tests (BNP or NT-proBNP levels). Changes to biomarkers in your blood occur before changes in Functional Class and 6-minute walk distance, and changes in Functional Class and 6-minute walk distance occur before hospitalization.
Echocardiograms can monitor how the heart is changing
PAH specialists now understand how important it is to monitor the right side of the heart frequently. An echocardiogram (Echo) can be used to catch any changes early and also to see how you are responding to your treatment plan. This is why Echos are so important.
How often should I get an Echo?
Echos are recommended at least twice a year for many patients with PAH.
Echo: Getting to the heart of the matter
Take a look at how PAH specialists use the Echo as a noninvasive test to monitor changes in the right heart. Learn more about how the results from your Echo can help guide you and your doctor to take action.
PAH Today: Echo – Getting to the Heart of the Matter
Lana Melendres-Groves, MD:
[on-screen text: Lana Melendres-Groves, MD, Medical Director, Pulmonary Hypertension Program] So, when we talk about an echocardiogram, what we’re looking at are all of the different chambers in the heart. So, we have four muscle chambers. We have two chambers on the right side of the heart that are depicted in blue, and we have the two chambers on the left side of the heart depicted in red. I also break it down into the two smaller chambers, which are sort of on the top of the heart, called the right and left atrium, or the two larger chambers that sit below those small chambers called the right ventricle and left ventricle. With the Echo, we’re able to look at the size of the chambers of the heart, we’re able to tell by the shape of them and how they squeeze and the thickness of the muscles how the heart may be doing overall and how it’s functioning. This can change with therapies, and so therefore, we can use it as an evaluation to a response to a therapy.
So, let’s go ahead and look at an Echo. Well first, we have to let you know that we actually flip the heart upside down when we look at it, so we took the picture from the prior slide and flipped it upside down. So, this is how we really look at it when we look at an Echocardiogram. It’s flipped upside down, so now those larger chambers, the ventricles, are sitting toward the top, as you can see, and those smaller chambers are sitting toward the bottom of the screen. Now I know, it’s a lot of kind of black, white, and gray, so hopefully you’re able to sort of see that within those white areas are the chambers of the heart, and the black area is where the blood would be moving through. You can see that the arrows show the distance between the walls of the right ventricle and the left ventricle, and you may note that the right ventricle is smaller than the left ventricle, and that is completely normal for a patient who does not have PAH.
We also look at what we call the apex of the right ventricle. So, it’s kind of the point of it, and it usually is very thin-walled, and because the right side of the heart is under low pressures in a normal situation, the walls of the muscle don’t have to be thickened. We also can see that the right atrium and left atrium are about the same size. This, again, is in a person who does not have PAH.
So, what happens to the heart in a patient with PAH? Well, let’s go ahead and take a look at a side by side of a patient with an advanced or severe pulmonary arterial hypertension, PAH, and then somebody who does not have PAH. You can see that they look pretty dramatically different. You can note that the area of the right ventricle of the patient without PAH starts to become much more enlarged when somebody has advancing PAH. You can also see that the left ventricle seems to be shrinking in size. Well, it’s not technically shrinking, it’s just being kind of pushed over because the right ventricle and the left ventricle share that middle wall, so as the right ventricle starts to enlarge, it pushes into the wall, kind of squishes the left side of the heart. You may also notice that the right atrium has become substantially enlarged, especially compared to the left atrium. There are many other aspects that we also look at when determining how advanced someone’s PAH is that we won’t go into today, but again, are things that you may feel interested in and want to learn further about.
So, in this situation, what we look for is a patient with PAH having a right ventricle that is larger than normal. We also look for thickening of the muscle at that point or apex of the right ventricle, and we tend to see that the right atrium is enlarged.
[on-screen text: Monitoring the right heart with Echo helps healthcare providers be proactive with treatment and try to prevent symptoms before they happen. Symptoms worsen after changes in the heart occur.] So again, coming back to this graph, those changes in the heart help us to proactively understand what might be coming from a clinical side of it, meaning how you feel and what you’re able to do. And so, instead of waiting until someone feels those symptoms, we can use an echocardiogram to act more urgently on their behalf. We don’t ever want to see our patients’ symptoms worsen to the point that they may require hospitalization.
Monitoring your right heart is a crucial part of understanding the bigger picture of your PAH
Learn more about what your right heart health reveals about your PAH risk status.
PAH Life Expectancy & Risk Status