
Frequent risk assessments inform treatment decisions
According to today’s treatment recommendations, patients with pulmonary arterial hypertension (PAH) should receive an objective, multiparameter risk assessment at diagnosis and follow-up risk assessments as often as every 3 months thereafter.1,2
These risk calculation tools can help you quickly calculate your patient’s risk score with point-and-click ease. You can choose from among 5 calculators.
Use these online tools to calculate your patient’s risk status and help inform initial and follow-up treatment approaches
At diagnosis
REVEAL 2.0
2022 ESC/ERS Treatment Guidelines
During follow-up
REVEAL Lite 2
COMPERA 2.0: 4‑Risk Strata
French Noninvasive Criteria
How to use calculator tools:
Download Instructions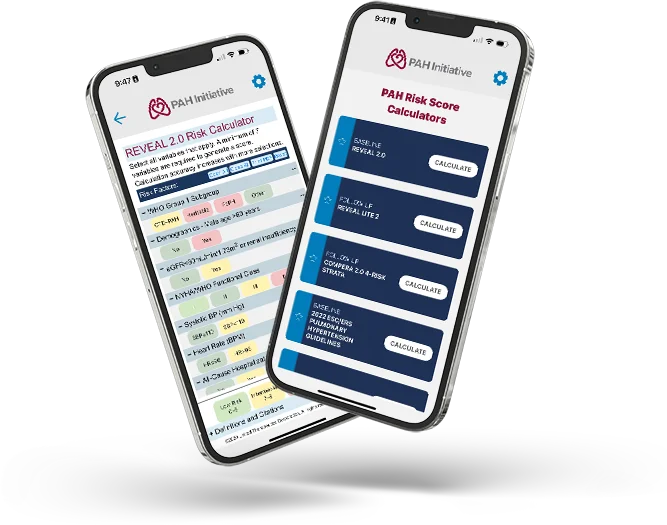
PAH Initiative Risk Score Calculator App
PAH Initiative has created a Risk Score Calculator App to assist in calculating risk scores using guidelines and other methodologies. Explore this exciting new tool
Download Risk Calculator AppDiscuss risk with your patients
Help your patients become more invested in achieving low risk. Use the handouts below to facilitate conversations with your patients.

Risk Calculator Worksheets
Download this PDF for a copy of the of REVEAL 2.0, REVEAL Lite 2, 2022 ESC/ERS Treatment Guidelines, and COMPERA 2.0 4-Risk Strata calculation methods

Patient Risk Infographic
Use this infographic to help your patients understand the importance of improving their risk status
PAH Monitoring Guide
Review key elements of monitoring risk status and right heart parameters in your PAH patients